Koorosh Ahmadi1,
Hossein Zakeri2,
Hamid Zamani Moghadam Doloo2,
Behrang Rezvani Kakhki2,
Ali Mohammadshahi3,
Mostafa Alavi-Moghaddam4,
Amir Masoud Hashemian2 ![]()
For correspondence:- Amir Hashemian Email: HashemianAM@mums.ac.ir Tel:+989124244517
Received: 15 December 2015 Accepted: 22 March 2016 Published: 30 April 2016
Citation: Ahmadi K, Zakeri H, Doloo HZ, Kakhki BR, Mohammadshahi A, Alavi-Moghaddam M, et al. Multi-drug resistant Staphylococcus aureus isolated from emergency ward of an Iranian hospital. Trop J Pharm Res 2016; 15(4):815-819 doi: 10.4314/tjpr.v15i4.21
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
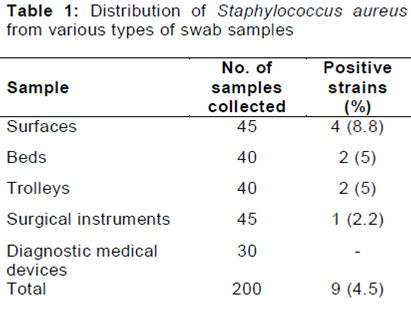
Purpose: To study the prevalence of resistant strains of S. aureus isolated from surfaces, beds and various equipment of an Iranian hospital emergency ward.
Methods: Two hundred swab samples were collected from the surfaces, beds, trolleys, surgical equipment and diagnostic medical devices in emergency ward. Samples were cultured and those that were S. aureus-positive were confirmed using polymerase chain reaction (PCR). Antimicrobial resistance pattern was analyzed using disk diffusion method.
Results: Nine of 200 samples (4.5 %) collected were positive for S. aureus. Surfaces (8.8 %), beds (5 %) and trolleys (5 %) were the most commonly contaminated. S. aureus isolates exhibited varying levels of resistance against antibiotics with the following being the highest: tetracycline (88.8 %), penicillin (88.8 %) and ampicillin (77.7 %). The prevalence of resistance against methicillin, oxacillin and azithromycin were 44.4, 33.3 and 33.3 %, respectively. There was no pattern of resistance against imipenem.
Conclusion: Efficient disinfection of surfaces, beds, trolleys and surgical instruments should be performed periodically to reduce colonization of resistant strains of S. aureus in various areas of emergency health care centers.
Introduction
Emergency health care centers of hospitals are often full of patients with critical and emergency situations. These patients are mainly the sources of dangerous pathogenic bacteria. Therefore, disinfection of surfaces, beds, equipment and facilities of the emergency health care centers can help to prevent the spread of bacterial strains which are mainly resistant to majority of antibiotics. High numbers of accident cases referred to hospitals and also lack of attention to hygienic principles can result in the occurrence of air-borne infections in hospital environment.
Staphylococcus aureus (S. aureus) has long been considered as a major pathogen of hospital infections all-around the world. It has been associated with bacteremia, infective endocarditis and various types of infections including skin and soft tissue, osteoarticular, pleuropulmonary, urinary tract and device-related [1-3]. The ability of S. aureus to develop resistance to certain environmental conditions and also wide range of antibiotics and disinfectant agents. Bacteria have been implicated as a cause of long-term survival pathogens in the environment [4].
High capability of S. aureus to develop resistance to most antibiotics, has caused problems in the treatment of hospital infections. It has been documented that majority of S. aureus strains were resistant to oxacillin, ampicillin, methicillin, penicillin, tetracycline, co trimoxazole, azithromycin, cefexim and clindamycin [5-7]. In recent years prevalence of resistance against several types of antibiotics has increased throughout the world [5-8]. Methicillin-resistant S. aureus (MRSA) has caused substantial public health problem worldwide, with significant morbidity, mortality and high cost of health care [9]. There was an estimated 94,360 invasive MRSA infections in the United States in 2005, causing more than 18, 000 deaths per year [10].
Due to inadequate hygienic conditions of Iranian emergency health care centers, the present investigation was carried out in order to determine the prevalence of multi-drug resistant S. aureus isolates from the environment and equipment of the centers.
Methods
Sample collection
A total of 200 swab samples were directly collected from various parts and equipment of emergency health care centers including surfaces (n = 45), beds (n = 40), trolleys (n = 40), surgical instruments (n = 45) and diagnostic medical devices (n = 30). All samples were immediately transferred to the laboratory at 4 °C in a cooler with ice packs.
Staphylococcus aureus identification
All samples were directly cultured into 7 % sheep blood agar (Merck, Darmstadt, Germany) and incubated aerobically at 37 °C for 48 h. After incubation, suspicious colonies were examined by the use of morphologies compatible with Staphylococcus spp. (microscopical morphology, catalase and coagulase production). Studied colonies were cultured on Tryptic Soy Broth (TSB) (Merck, Darmstadt, Germany) and Tryptic Soy Agar (TSA) (Merck, Darmstadt, Germany). After growth, staphylococci were identified on the basis of colony characteristics, Gram staining, pigment production, hemolytic and the following biochemical reactions: catalase activity, coagulated test (rabbit plasma), Oxidase test, glucose O/F test, resistance to bacitracin (0.04 U), mannitol fermentation on Mannitol Salt Agar (MSA) (Merck, Darmstadt, Germany), urease activity, nitrate reduction, novobiocin resistance, phosphatase, deoxyribonuclease (DNase) test and carbohydrate (xylose, sucrose, trehalose and maltose, fructose, lactose, mannose) fermentation test [11].
Antimicrobial susceptibility test
Pattern of antimicrobial resistance was studied using the simple disk diffusion technique. The Mueller–Hinton agar (Merck, Germany) medium was used for this purpose. Antibiotic resistance of S. aureus strains against 15 commonly used antibiotics in the cases of UTIs was determined using the instruction of Clinical and Laboratory Standards Institute guidelines [12]. Susceptibility of S. aureus isolates were tested against ampicillin (10 u/disk), imipenem (30 u/disk), methicillin (30 µg/disk), tetracycline (30 µg/disk), norfloxacin (30 µg/disk), cotrimoxazole (30 µg/disk), clindamycin (2 µg/disk), penicillin (10 u/disk), oxacillin (1 µg/disk), azithromycin (15 µg/disk) and cefexime (5 μg/disk) antibiotic agents (Oxoid, UK). The plates containing the discs were allowed to stand for at least 30 min before incubated at 35 °C for 24 h. The diameter of the zone of inhibition produced by each antibiotic disc was measured and interpreted using the CLSI zone diameter interpretative standards (CLSI 2012) [12]. S. aureus ATCC 43300 and K. pneumoniae ATCC 4352 were used as standard organisms in antimicrobial susceptibility determination.
DNA extraction and PCR confirmation
Total genomic DNA was extracted from the bacterial colonies using the genomic DNA extraction kit (Fermentas, Germany) according to the manufacture instruction. The DNA concentration was determined by measuring absorbance of the sample at 260 nm using spectrophotometer [13]. Presence of S. aureus in each DNA samples was confirmed using the Daniel et al [14] method. The PCR reaction mix consist of 1 X PCR buffer (10 mM Tris-HCl, pH 8.3, 50 mM KCl and 0.001 % (w/v) gelatin) with 4 mM MgCl2, 250 mM of each nucleotide (deoxynucleoside triphosphate), 0.5 mM of each primer (F: 5’-GGAATTCAAAGGAATTGACGGG G GC-3’ and R: 5’-CGGGATCCCAGGCCCGG GAACGTATTCAC -3’) (479 bp size of product for 16S rRNA gene of the S. aureus), 4 ng of the molecular beacon and 4 U of Jumpstart Taq DNA polymerase (Fermentas, Germany).
Statistical analysis
Data were entered into Microsoft Excel spreadsheet (Microsoft Corp, Redmond, WA, USA) for analysis. Using SPSS 16.0 statistical software (SPSS Inc., Chicago, IL, USA), Chi-square test and Fisher’s exact two-tailed test analysis were performed and differences were considered significant at p < 0.05. Distribution of S. aureus and antibiotic resistance pattern were statistically analyzed.
Results
A total of 200 swab samples obtained from various sites of emergency health care centers were analyzed for presence of S. aureus. shows the distribution of S. aureus in various types of swab samples. Of 200 swab samples studied, 9 samples (4.5 %) were positive for S. aureus. Swab samples which was collected from the surfaces of emergency health care centers was the most commonly contaminated (8.8 %), followed by beds (5 %) and trolleys (5 %). Statistically significant difference was seen for the prevalence of S. aureus between the samples collected from surfaces and surgical instruments (p = 0.021) and also beds and surgical instruments (p = 0.039). There were no positive results for the swabs taken from diagnostic medical devices. The results of culture technique were also confirmed by the PCR method. shows the results of the gel electrophoresis for the identification of 16S rRNA gene of the S. aureus strains.
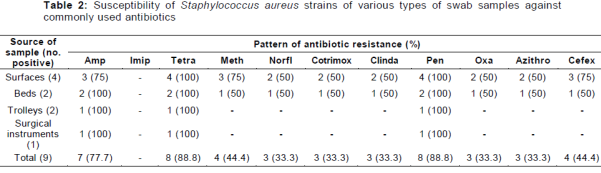
shows the antibiotic resistance pattern of the S. aureus strains isolated from the swab samples taken from various sites of the emergency health care centers. We found that the S. aureus strains were resistant to tetracycline (88.8 %), penicillin (88.8 %) and ampicillin (77.7 %). The prevalence of resistance against methicillin, oxacillin and azithromycin were 44.4, 33.3 and 33.3 %, respectively.
However, the isolates were susceptible to imipenem. S. aureus strains of surgical instruments and trolleys had the highest levels of resistance. Statistically significant differences were seen between the resistance against tetracycline and oxacillin (p = 0.019), tetracycline and methicillin (p = 0.028), penicillin and clindamycin (p = 0.023) and penicillin and methicillin (p = 0.030).
Discussion
The results of the present investigation revealed the low incidence (4.5%) of resistant strains of S. aureus in various sites and equipment of the emergency health care centers of Iranian hospitals. Despite the low incidence of S. aureus, the public health implications cannot be downplayed in emergency care centers. One possible explanation for presence of S. aureus could be that the emergency health care centers is the fact that the environment of the emergency health care centers was heavily contaminated. It may also be indicative of improper and inadequate disinfection of surfaces and equipment. Reports showed that S. aureus survived adverse situation like high levels of acidity, dryness and salty conditions [15-17], and hospital environment [18-20].
In a study by Alebachew et al [21], the S. aureus strains of human clinical infections were sensitive to clindamycin, vancomycin, erythromycin, and kanamycin but highly resistant to penicillin. They showed that all isolates were multi-drug resistant, and one isolate was resistant to all the tested drugs. In a research in Iran [22], 60 % of all S. aureus isolates of hospital infections were resistant to methicillin. Ekrami et al [22] showed that the highest resistance was to ciprofloxacin (81.2 %) while Momtaz and Hafezi [23] found that S. aureus isolates from hospital infections were resistant to azithromycin (62.12 %), tetracycline (57.57 %) and erythromycin (54.54 %).
S. aureus strains obtained in this study were fully susceptible to imipenem, moderately susceptible to norfloxacin, cotrimoxazole, clindamycin, oxacillin and azithromycin antibiotics. Similar results have been reported previously [21-23]. Methicillin was one of the first lines of drugs for the chemical management of S. aureus infections. The resistance against this antibiotic in this study was 44.4 %. Important role of methicillin resistant S. aureus (MRSA) as causative agent of human clinical infections has been reported previously [21-25]. The observed antibiotic resistance in our study maybe due to the moderately high prescription of methicillin in Iranian health center and hospitals. In addition, this finding may be reflective of the possible failure of internal disinfection process in the hospital’s environment.
Conclusion
The results of the present investigation indicate that S. aureus might be an important causative agent of nocosomial infections in emergency centers of hospitals. Accurate and continuous surveillance of antibiotic resistance patterns among S. aureus strains should be considered in emergency health care centers. Prescription of imipenem for the treatment of cases of S. aureus is recommended. Effective disinfection of surfaces, beds, trolleys and surgical instruments by hospital infection control unit should be performed periodically to reduce colonization of S. aureus in various areas of hospital emergency wards.
Declarations
Acknowledgement
References
Archives


News Updates